Looking for information about other Dental Topics?
Full Website Index• Animated-Teeth.com •

Dental Bonding- Use cases with front teeth.
Utilizing dental bonding with front teeth.
Dental composite, the material used with tooth-bonding technique, is unique in two ways:
- It mimics the color and appearance of tooth enamel well.
- It’s able to adhere directly to a tooth’s surface (even a smooth flat one).
- 1) White fillings.
- 2) Correcting minor tooth imperfections.
- 3) Closing tooth gaps.
- 4) Composite veneers.
- How long can bonded restorations last?
- How they compare to other types of restorations placed on front teeth, like porcelain veneers.
A front tooth with a cavity.

Dental composite is the restorative most used to create fillings for front teeth.
A) White fillings.
Alternatives.
Although it does have shortcomings (see disadvantages below), for teeth where a simple, conservative, natural-looking repair is needed there is no alternative.
Details.
This page outlines the steps a dentist follows when placing bonding. This exact same process is used with each of the other applications listed on this page.
FYI –Using dental composite to make white fillings for front teeth is standard and routine. Using it to create white fillings for back teeth is an entirely different matter. We discuss that issue here.
Because it’s able to bond directly to tooth enamel …

.. dental composite makes the ideal restorative for making minor tooth repairs.
B) Minor cosmetic improvements.
Alternatives.
Details.
In some cases, the needed repair can be astoundingly easy. Possibly as simple as bonding a layer of composite directly over the offending area, without even having to trim the tooth first.
Notes.
With this and the remainder of applications listed on this page, the use of a dental anesthetic may not be needed when the bonding is placed.
That’s because the necessity for anesthetic typically hinges on the amount of tooth trimming that’s required. If little to none is needed, then it’s likely that anesthetic won’t be needed either.
C) Filling in gaps between teeth.
Dentists use the term “diastema” to refer to a space between two front teeth.
From a standpoint of function and dental health, these gaps pose no problem. But in regard to cosmetic appearance, some people find them unappealing. For those who do, bonding can provide a solution.
Dental bonding makes a good choice for closing relatively small tooth gaps.
The space is closed in by adding an equal width of composite to each tooth.
Alternatives.
Porcelain veneer placement would be the most common alternative to closing a gap with bonding. We compare the advantages and disadvantages of each below.

A case where bonding could be used to close a tooth gap (diastema).
Details.
Since the underlying goal is increasing the size of the tooth, it’s likely that no tooth trimming will be required. If so, no other way of closing a gap is as minimally-invasive as this.
Notes – 1.
Notes – 2.
Porcelain veneers are made by a technician in a dental laboratory, as opposed to right on the tooth like with dental bonding.
And for that reason, with difficult cases (like closing very large gaps) it may be easier to obtain ideal restoration contours via placing a veneer.
D) Dental composite veneers.
Similar to porcelain veneers, a dentist can use dental composite to create a covering (veneering) for the entire front surface of a tooth. In fact, the technique of placing composite veneers predates the porcelain procedure by several decades.
Details.
In strictly cosmetic applications, the goal of this procedure is to resurface the tooth (so its appearance is improved) without significantly increasing its thickness. That means the dentist may need to trim back the tooth’s front side somewhat before placing the bonding. If so, the use of an anesthetic may be required.
Veneers are used to resurface the visible portion of a tooth.
Notes.
- When a porcelain one is made, the dentist takes an impression of the prepared tooth. A dental laboratory technician then uses it to fabricate the veneer.
- In comparison, with composite veneers it’s the dentist who is the artisan. And unlike a dental technician who is working in a laboratory environment at their leisure, a dentist has to achieve their results right there during the dental appointment, within the amount of time that has been allotted.
It’s no small feat for a dentist to create a veneer out of dental bonding that is both beautiful and functionally correct.
How long will bonded restorations on front teeth last?
All dental composite restorations have the potential to stain (see below). And for larger restorations, wear or fracture can become an issue.
We found several studies that evaluated the longevity of relatively larger restorations (those used to close tooth gaps and/or resurface and reshape teeth). [page references]
A picture of a deteriorated dental composite filling.
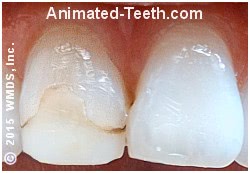
Its entire front surface has worn. Its edges have stained.
- Frese (2013) reported that at the 5-year mark roughly 15% of the 175 restorations followed required some type of repair (none were completely lost, all could be repaired). Of the restorations that didn’t experience some type of failure, 90% were rated as clinically good or excellent at 5 years.
- Wolff (2010) followed 327 composite restorations. This paper determined an 80% 5-year survival rate. Most of the repairs needed were related to minor fractures of the bonding. One restoration was lost totally. Like above, of the restorations that didn’t experience some type of failure, 90% were rated as clinically good or excellent at 5 years.
- A literature review by Wakiaga (2004) reported a 74% 2-year survival rate for composite veneers vs. 94% for porcelain.
▲ Section references – Frese, Wolff, Wakiaga
FYI –Comparatively smaller composite restorations will likely have a longer lifespan than those evaluated in the studies above. But even if not, bonding still makes the right choice when just a small restoration or repair is needed.
When relatively larger restorations are required (veneers, very large fillings), discuss possible alternatives with your dentist. While their initial cost may be more, due to their greater longevity other procedures (crowns, porcelain veneers) may prove to be more cost-effective.
Advantages and disadvantages of composite restorations over porcelain ones.
Some of the applications for dental bonding for front teeth could instead be treated via the placement of porcelain veneers or crowns.
When trying to decide between these alternatives, here’s a list of general advantages and disadvantages to consider.
A) Bonding is usually less expensive.
Dental composite restorations usually cost less than porcelain ones.
- They’re placed in just one visit whereas porcelain restorations require two appointments (and therefore more appointment time).
- With porcelain restorations, there’s a bill from a dental laboratory for fabricating it.
B) Bonded restorations can be repaired if they break.
If a large composite filling or veneer does chip or break, a dentist can almost certainly repair it. And in most cases, they can probably make the repair by just patching the damaged part.
In comparison, while a patch or repair may be possible in some cases, if a porcelain restoration breaks it will likely need to be replaced.
C) Composite restorations will show wear.
Dental composite is a plastic compound. And although manufacturers add components to enhance wear resistance, it still occurs.
A person may notice that over time the outline shape of their bonding has changed (especially on its biting edge). In comparison, porcelain is harder, and therefore will hold its original form better over the long term.
Stained white fillings.

Polishing, resurfacing or replacement might each be options.
D) Bonding can be expected to stain.
As a fix, it might be possible that just polishing the surface of the bonding will restore it to its original appearance. In other cases, the dentist may feel they need to trim off the entire front side of the restoration and resurface it with a new layer.
D) Porcelain restorations tend to look more natural.
How porcelain veneers handle light.
Light penetrates into the veneer and then reflects back out.
What creates luster?
And the way light is able to enter into this layer and then reflect back out is what creates the glass-like luster that we typically associate with tooth enamel. (This page gives a more detailed explanation.)
How dental composite restorations handle light.
Light primarily reflects off the front surface of the bonding.
How dental bonding handles light.
E) Gum tissue concerns.
At least in theory, porcelain restorations may be more advantageous in terms of maintaining gum health.
Dental composite can’t be polished down to the same high degree of surface smoothness as porcelain. As a result, it will tend to retain more food debris and plaque (Jacobson 2008). However, in the case where effective oral home care is practiced regularly, this issue shouldn’t pose a significant problem.
Which should you choose?
In instances where cost is not an issue (like the case where a dentist is placing a restoration for a family member), it’s fairly safe to assume that most dentists would typically choose to place porcelain veneers and crowns as opposed to their dental composite alternatives.
And while we don’t know the exact criteria involved, the literature review mentioned above (Wakiaga 2004) reported “patient satisfaction” rates of 67% for composite veneers vs. 93% for porcelain ones (based on the evaluation of 200 restorations over a time period of 2.5 years).
Last reviewed: September 21, 2019
Author: Paul Cotner, DMD — retired dentist.
Published by: WMDS, Inc. — owner of Animated-Teeth.com.
Educational information only — not a substitute for professional dental care.
Page references sources:
Frese C, et al. Recontouring teeth and closing diastemas with direct composite buildups: a 5-year follow-up.
Wakiaga J, et al. Direct versus indirect veneer restorations for intrinsic dental stains.
Wolff D, et al. Recontouring teeth and closing diastemas with direct composite buildups: a clinical evaluation of survival and quality parameters.